We are trained to look and observe for any oral habit that may be occurring with your child and to suggest steps necessary to prevent oral habits from causing any long term ill effect with your childs dental health and development.
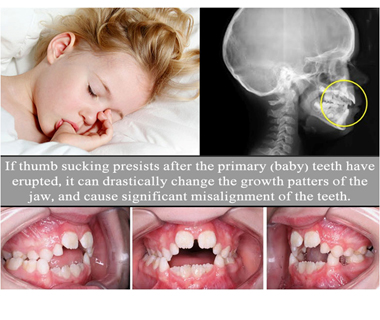
Thumb and finger habits make up the majority of oral habits. However two thirds of children who engage in thumb and finger habits outgrow them by age five. The dentofacial changes will vary with the intensity, duration and frequency of the habit and the position of the digit in the mouth. The dentofacial changes include:
The earlier the habit is discontinued the greater the likelihood of dentofacial changes self correcting. However, the child should be allowed to stop the habit spontaneously. Most habits stop in school due to peer pressure so definitive treatment is not initiated until ages 4-6 years. If the child or the parent does not want to discontinue the habit do not force the issue. The type of treatment prescribed is dependent on the childs willingness of the child to stop the habit.
Lip licking is the most common lip habit. The most common clinical effects are inflamed chap lips exhibiting an erythematous wide border encircling the lips with normal skin area just around the vermillion border. Severe lip licking, with the lower lip tucked behind the maxillary incisors, places excessive lingually directed forces on the mandibular teeth and facial forces on the maxillary teeth, resulting in retro-inclination of the mandibular incisors, proclination of the maxillary incisors and increased overjet. Appliance can be given to stop the habit and the irritated areas can be controlled with the application of steroids, antibacterial and antifungal.
Bruxism is the nonfunctional grinding or gnashing of teeth. It occurs most often during sleep, however some children grind their teeth when awake. It results in wear of teeth and can cause masticatory muscle soreness and TMJ pain. Local factors include occlusal interferences or high restorations. Systemic factors include stress, personality disorders, nutritional deficiencies, allergies, endocrine disorders, musculoskeletal disorders and mental retardation. Most children outgrow the habit and treatment is unnecessary. For those that do not, treatment consists of:
Although mouth breathing is common and sometimes overlooked, it is a primary cause of facial and dental deformities and irregularities. Mouth breathing is caused by chronic nasal obstruction (CNO). No one breathes through the mouth as a habit. Children rarely complain of mouth breathing because they quickly accept it as their “normal.” Dental and facial deformities / irregularities can be prevented or minimized by timely and appropriate treatment.


